- Useful for lower abdominal, perineum, lower extremity surgery
- Avoid in:
- Patients in shock, not yet fully resuscitated
- Infection at site of spinal needle placement
- Frank coagulopathy
- Patient refusal
- Convulsion or raised intracranial pressure due to brain tumour
- Preload patient with 500-1000 ml of normal saline
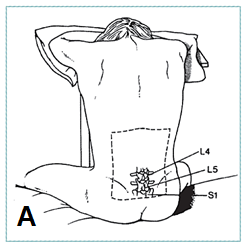
- Position patient in sitting (A) or lateral position
- Prepare lower spinal area carefully
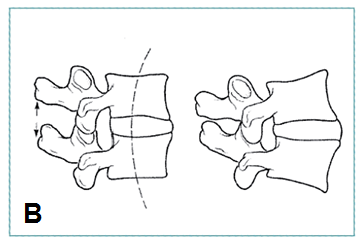
- Have patient maximally flex lower spine to open intraspinous space (B)
- Point of needle entry should be between L4-L5 or between L5-S1
|
  |