|
Insert retention sutures through entire thickness of abdominal wall leaving them untied (A)
Simple or mattress sutures
Close wound in layers (B)
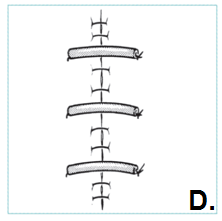
When skin closure completed, tie each retention suture after threading through short length plastic or rubber tubing (C, D)
Do not tie retention sutures under tension
Leave sutures in minimum 14 days; may be left for weeks
|
 |