FEMALE GENITAL MUTILATION
- There are NO health indications for female genital mutilation
- Acute complications:
- Haemorrhage
- Shock
- Urinary retention
- Damage to urethra, anus
- Cellulitis
- Abscess formation
Treatment:
- Wound debridement, saline irrigation, remove all foreign material
- Remove minimal tissue, drain abscess
- Antibiotics for infected wounds, cellulitis, abscess
- Catheterize bladder
- Tetanus toxoid if non-immune
- Excise epidermal tissue, if present, to permit urinary flow and sexual intercourse
Chronic complications include:
- Sexual dysfunction, dyspareunia
- Psychological disturbance
- Urinary obstruction
- Keloids
- Large epidermal inclusion cysts
- Difficult urination
- Vaginal stenosis; may cause obstructed labour, often complicated by vesico- or recto- vaginal fistulae
DELIVERY IN THE PRESENCE OF INFIBULATION
Vaginal closure due to type III female genital mutilation
- Women with type III FGM – infibulation need to be opened for childbirth to reduce the risk of serious tears and obstructed labor.
- The first choice should be defibulation, opening of the infibulated scar, which is a less infringing procedure than episiotomy, as the seal of skin covering the vagina is usually thin with few nerves and blood vessels
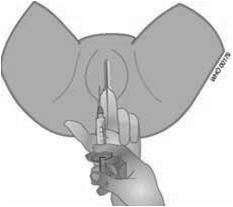
- Infiltrate 2-3 ml of local anesthetics into the area where the cut will be made, along the scar and in both sides of the scar
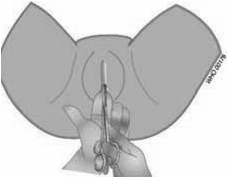
- With your finger or dilator inside the scar, introduce the scissors and cut the scar alongside the finger or fingers to avoid injury to the adjacent tissues
- The cut should be made along the mid-line of the scar towards the pubis
- Incise the mid-line to expose the urethral opening
- Review whether episiotomies will also be necessary to avoid tearing
- After childbirth, suture the raw edges separately using fine 3/0 catgut to secure hemostasis and prevent adhesion formation
|

 |